


 Artículos originales> Expertos del Mundo>
Enviar correspondencia a:
Patrocinio y reconocimiento
Artículos originales> Expertos del Mundo>
Enviar correspondencia a:
Patrocinio y reconocimiento
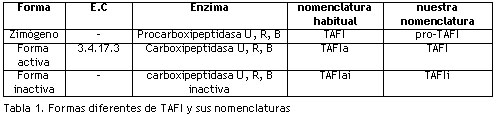
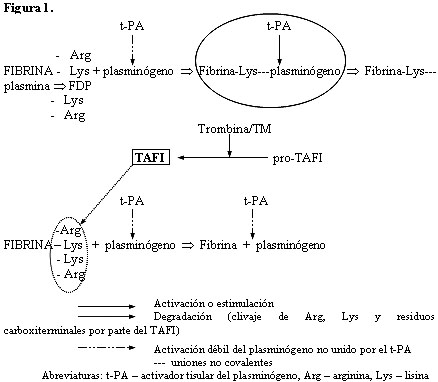
Figura 1. Presentación simplificada del papel de TAFI en la fibrinólisis (de Antovic61; con autorización de Clinical Laboratory, Heidelberg, Alemania).Medición de las diferentes formas de TAFI
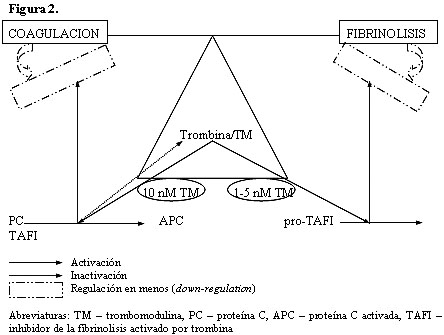
Figura 2. Presentación simplificada del efecto de trombina/trombomodulina en la coagulación y fibrinólisis (de Antovic61; con autorización de Clinical Laboratory, Heidelberg, Alemania).La formación defectuosa de trombina induce una tendencia al sangrado en pacientes con deficiencias heredadas de los factores de la coagulación. Las cantidades de TAFI podrían aportar una explicación aceptable para la regulación positiva de la fibrinólisis en pacientes con deterioro en la formación de trombina. Se observó que los coágulos formados a partir de plasmas con deficiencias en los factores VIII, IX, X y XI se lisan de manera prematura y que la suplementación con factores corrige este defecto y al mismo tiempo incrementa la tasa y la extensión de la activación de la carboxipeptidasa U (TAFI). El agregado de factor VIII restauró la fibrinólisis en plasmas provenientes de personas con hemofilia A. La inyección de rFVIIa normaliza la hemostasis general y la fibrinólisis dependiente del TAFI en pacientes con hemofilia A e inhibidores, mientras que la adición in vitro de rVIIa en plasmas con deficiencias de diversos factores normaliza la hemostasis global y, al menos en parte, la fibrinólisis dependiente del TAFI.